Trump Cuts Obamacare Outreach Funding Again
Trump's advertizing cuts will cost a minimum of 1.1 million Obamacare enrollments
The Trump administration recently announced that they were cutting the outreach and instruction budget for Obamacare past xc percent, from $100 million to $10 million. As the person in charge of how that money was spent last yr, I decided to crunch the numbers to figure out what that would mean for enrollment this yr.
A minimum of ane.1 one thousand thousand fewer people will enroll in the federal exchange solely because of the administration's drastic cuts to Open Enrollment outreach. Go on in mind, this is the least harm the administration's outreach cuts could have — this is a best case scenario. Information technology assumes they spend the $x meg they have budgeted well and that nada else the administration has washed will affect enrollment. For example, this estimate doesn't account for consumer confusion near repeal efforts, the Executive Order or the end of payments of Cost Sharing Reductions.
When it comes to estimating the impact of outreach, I am non pulling a number out of the air. The administration falsely asserted that "they had non done any studies of the efficacy of enrollment advertising". This is absurd. The Department of Health and Human Services closely measured the impact of outreach during previous Open Enrollments so nosotros have a articulate understanding of how constructive advertisement is at driving enrollment. Internal HHS reports, written nearly past the Huffington Post, documented a ii-twelvemonth study of the causal human relationship between outreach and enrollment.
Surprise: advertising works!
But the research tells us more than but the fact that it worked. It tells u.s.a. what worked and how many enrollments were generated per dollar spent.The HHS report shows that television, radio, digital ads, search advertisement, emails, phone calls, mobile ads, direct mail, and more bulldoze enrollment. It'southward also part of the reason HealthCare.gov had its biggest day of enrollment ever last yr.
Using the research, nosotros tin can roughly quantify how enrollment will be impacted this year. I did this in one case before, when the Trump administration cut outreach during the final week of Open Enrollment in January 2017. Earlier those cuts took consequence, I said that decision would likely cost 500,000 people coverage — and looking at the final enrollment numbers, that seems pretty shut. Nearly 500,000 fewer people enrolled at the end of January compared to the equivalent time catamenia the previous year and in my post I highlighted why enrollment at least had the potential to be even college than the previous year. This bluish and red in this ACASignUps.net graph show just how dissimilar the final week of Jan was compared to the previous year.
The threat to Open Enrollment this year is very real. People volition be injure by the assistants'south deportment. But we aren't powerless either.
Lori Lodes and I founded Get America Covered, because we recognized that the administration intended to do and then little — they'd set the bar and so depression — that a committed group of people could brand a big difference. The same free energy that stopped repeal efforts has the potential to change the course of Open Enrollment. Together, we can Get America Covered.
Desire to help? Find out how!
If you're interested, I walk through how I arrived at the i.1 million enrollments below.
Methodology
Assumptions
This time, given the severity of the cuts to advertising and outreach and the sheer number of things that are changing I'g working off a few assumptions.These assumptions underscore why this estimate is a best example scenario and that it likely underestimates the impact of outreach cuts on enrollment. Here's what I'm assuming:
- Other changes to Open Enrollment and the ACA will not negatively bear on enrollment.
- No change to the underlying uninsured population. New Gallup data suggest this may not be true, but factoring this into the analysis would be significantly more than complicated.
- HHS selects the most efficient outreach tactics they can afford during Open Enrollment. While still theoretically possible, it's unlikely.
- HHS uses all-time practices when they carry outreach. With years of testing, we know what'southward helpful to become people enrolled and what'southward not. At that place is almost no risk HHS will use best practices. For example, the administration stopped mentioning the penalty for not having coverage in about all consumer communication last twelvemonth days after they they took over.
- The administration is retaining customers at the same charge per unit we did. While probable not true, I assume this assistants has been working just as hard to keep current consumers happy between open enrollments and enrolling new customers at the same charge per unit.
Hypothetical Marketing Program
I created a hypothetical marketing program for HHS — this is the simple version of the program I'd write if I had a budget of $10 million to do outreach — it's a all-time instance scenario for outreach this year.
If I was asked to cut my $100 million budget to $10 1000000, nosotros'd start with some painful triage. I would eliminate all tactics that aren't 100% proven to drive enrollment. While that might seem like a good idea, this is extremely short-term thinking when y'all are responsible for a program of this size. You have to try new things (fifty-fifty if that means sometimes failing), because consumers and technology change every twelvemonth. If you terminate learning long enough, y'all increase your take a chance of running a program that loses efficiency and effectiveness each twelvemonth.
In past years, four tactics collection the vast majority of enrollment: Email, Phone Calls, National TV Ads, and Search Ad. For simplicity's sake, I am going to focus on these iv tactics though there are a few others that bulldoze smaller enrollment numbers, and would be relevant to the bodily programme.
Earlier we enroll anyone, nosotros take $1 meg off the elevation to pay for overhead (writing, graphic pattern, production, coming together regulatory requirements for data we work with, etc). Next, I'd optimize funding for the most toll-effective tactics.
- Reminder Emails and Calls: Together, email and phones are the most cost effective form of outreach responsible for roughly xxx% of outreach driven new enrollments and 45% of outreach driven active renewals straight attributable to outreach. Given their efficiency and importance, I'd do everything I could to support this outreach. Unfortunately, Open Enrollment is half the length compared to last year. While this doesn't modify the costs, it does reduce the impact via these channels. Where nosotros could prioritize re-enrollment last year, the aforementioned express resources (e.g. telephone calls to customers per day) would split our new vs returning consumer efforts. I'd still be forced to trim back some of the budget from the previous yr with the hope that year-over-year improvements might permit me to achieve similar functioning. I'd also demand to cut parts of the telephone programme that are more labor intensive for our call center team since they won't have the bandwidth to help additional customers given the condensed enrollment period that will drive much higher call center volume.
- Television receiver Ads: National TV was responsible for nearly 40% of enrollments directly owing to outreach — more whatsoever other single tactic. CMS already announced that they won't buy any national Boob tube (they can't possibly afford to). Every bit you can imagine, TV is one of the best ways to reach people who are not currently Marketplace consumers. Information from last year as well bear witness that TV nudged current consumers to actively renew their plans — lowering their premiums and increasing retention. TV increases the effectiveness of virtually every other tactic. As yous tin can imagine, people who come across a Idiot box ad are more probable to do a Google Search for "Obamacare", then meet a HealthCare.gov advertizement and\or sign-up for the HealthCare.gov email list.
- Search Advertising: Search Advertising lone was responsible for 25% of outreach driven new enrollments and eight% of active renewals. For simplicity sake, I'chiliad going to put all of what's left into search advertising — those ads that popup when you search for "health insurance". The more than complex program would split this amidst other digital ads also — but the bulk would exist in search. Unfortunately, all of what'south left (half-dozen million) is only 25% of last yr's Search Advertizement budget (the digital budget was even larger).
And just in case information technology's not obvious, fifty-fifty though email and phones were our most cost effective forms of outreach, we can't just increment these budgets. Unlike Goggle box and Search Advertisement, adding coin to Email and Phones has very limited bear upon on its ability to increase enrollment. For the near part, we're paying for infrastructure, not outreach. Sending email and making calls costs very little, but both tactics are dependent on people coming to HealthCare.gov and signing up. What's worse is that the two of channels that make people most likely to sign-upward to receive emails and phone calls are Goggle box ads and Search Ads, both of which face severe cuts this twelvemonth.
Hypothetical Budget
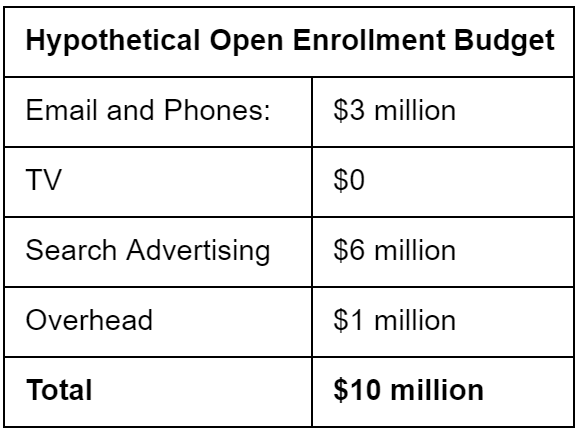
This budget is in sync with what HHS has publically announced (no TV or Radio instead they will use digital ads and continue to send email and text messages).
From Budget to Enrollments
From here, I use the measured impact of outreach past channel (East.k. TV, email, etc) final year and use it to the available budget. I eliminate new enrollments and active renewals generated past TV and cut the impact of search advertising to 25%. For email and phones, I demand to make two boosted assumptions, how many fewer new and returning enrollees will enroll because:
- Either they never sign up for the e-mail\phone lists considering they never saw a TV or digital advert and
- How many fewer will enroll equally a outcome of fewer outreach touches given halved Open Enrollment Period.
For returning consumers, my assumption is that email and phones will be 85% as constructive at getting consumer to renew their coverage — most of that reduction is attributed to the limits to the phone plan. For new consumers, I'm bold that email and phones will exist 60% every bit constructive as last year. This is a bigger reduction, but without Idiot box and the bulk of the digital advertizing budget, there will be far fewer people receiving emails or phone calls this twelvemonth. On acme of that, the team will have half the time to communicate within this shortened enrollment flow. This is likely a conservative approximate.
For the purpose of this exercise, I assume that everything else remains constant. What I get is a ballpark estimate of the expected impact of outreach for OE5.
Factors that are Not included in this assay
As a reminder, this assay doesn't account for the impacts to Open up Enrollment from the following (to proper noun a few):
- Consumer confusion due to repeal efforts, the Executive Order and the end of payments of Toll Sharing Reduction.
- Potential efforts to undermine the effectiveness of outreach during OE this includes:
a. Tactics: Not making smart decisions about how to spend the $10 1000000 upkeep.
b. Language: Not using tested language about how much coverage costs, what the penalization is or, for this year, highlighting that Open Enrollment is shorter and that the concluding deadline is on a new date entirely.
c. Personalization: Non using personalized outreach that speaks to an individual consumer's state of affairs (e.chiliad. if you don't shop, your premium will increase xxx%).
d. Frequency: Non following best practices established through testing on when and how often to remind consumers by email, phone, etc. - Confusion over when to sign up because of the new final deadline.
- Shortened enrollment catamenia.
- 41% cut to the in-person assistance navigator budget.
- Higher traffic due to a single enrollment deadline this yr volition create long client wait times at the telephone call centre and website and prevent frustrated consumers from enrolling.
- Lack of national and local media engagement by the administration before and during Open Enrollment.
- Non standing to appoint with businesses, libraries, country officials or other partners
- Assistants focus on falsely accusing the marketplaces of failing or imploding or making misleading statements nearly "soaring" premiums.
- HHS refusing to allow regional directors to assistance with state enrollment efforts.
- HHS actually using ACA funding to create and promote negative ads confronting the constabulary.
- Departed HHS and CMS staff who work on the ACA not being replaced.
- Less federal outreach that indirectly supports State Based Marketplaces or Medicaid (e.g. National TV).
- Lack of Special Enrollment Period email outreach and more arduous SEP verification steps for consumers mean fewer enrollees on November 1st.
It'southward pretty obvious that all of these will collectively hurt enrollment — together they may cause an even greater synergistic damage— it'southward only a question of how badly?
Results
In the best case scenario, where the most well-intended assistants imaginable spent the $ten million dollars in the almost efficient way possible, we'd expect to see merely shy of i one thousand thousand fewer new enrollments in the federal marketplace during the upcoming enrollment period.
In improver to this, we'd run into merely over a million fewer active renewals in the federal marketplace. Agile renewals matter a lot. Consumers who do not actively renew typically pay higher prices than those who do. It's non a surprise that they are far less likely to continue their marketplace coverage. Based on past beliefs, we tin wait an additional 200k consumers go out the Marketplace within 12 weeks of the terminate of Open Enrollment, because they did non actively renew.
Best Instance Scenario: Just 1.1 meg enrollments lost.
One other factor to keep in listen: The lost enrollments are probable to be disproportionately healthy people. In by years, we've seen that younger consumers and presumably healthier consumers are more likely to respond to outreach. As you can probably imagine, a patient with a chronic condition is typically more than highly motivated to enroll. Without outreach, the market will effectively lose 1.ane million of its healthier people.
Covered California's has outspent the Federal government on marketing for many years. They put out an analysis earlier this year, Marketing Matters: Lessons from California to Promote Stability, where they recommend that the federal government increase its marketing spend over final year substantially. They also note that i million fewer enrollments due to a decreased marketing spend is "likely a conservative estimate."
Source: https://medium.com/get-america-covered/trumps-ad-cuts-will-cost-a-minimum-of-1-1-million-obamacare-enrollments-9334f35c1626
0 Response to "Trump Cuts Obamacare Outreach Funding Again"
Post a Comment